In the operating room, visibility is synonymous with safety. While surgical instruments and robotic assistants often grab the headlines, the surgical shadowless lamp remains the surgeon's most critical tool. Without precise illumination, even the most skilled hands are rendered ineffective.
Today, medical lighting is undergoing a quiet transformation. The shift to LED technology is not merely an improvement in energy efficiency but a fundamental leap forward in optical performance, tissue safety, and infection control. But how does this LED shadowless lamp actually work? And what role do optical lenses play in it?
1. The Evolution of Surgical Lighting: From Halogen to LED
In the high-stakes environment of an operating room (OR), lighting is not merely a utility; it is a critical medical instrument. For decades, the industry relied on Tungsten Halogen technology. While these lamps served their purpose, they introduced significant physiological and operational risks that modern medicine can no longer tolerate.
The transition to LED Light technology represents completely redefining safety standards in surgical environments.
Hidden Risks of Halogen Lamps

Before LEDs became the standard, surgical lights were essentially high-powered heaters that happened to emit light. A halogen bulb works by incandescence—passing current through a filament until it burns white-hot.
While effective at generating brightness, this mechanism creates substantial Infrared (IR) Radiation. In a surgical context, this uncontrolled heat transfer poses serious clinical risks:
-
Tissue Desiccation (Drying): The most critical risk is the drying of exposed tissue. During long, open-cavity procedures (such as organ transplants or neurosurgery), the intense IR heat from halogen lamps can accelerate the evaporation of moisture from tissues. This desiccation can lead to cellular damage, delayed wound healing, and increased risk of post-operative complications.
-
The "Hot Head" Phenomenon & Infection Control: Halogen lights significantly raise the ambient temperature around the surgeon’s head and upper body. This causes surgeon fatigue and, more dangerously, perspiration. If a drop of sweat falls into the sterile field, the risk of a site infection increases dramatically.
-
Filament Fragility & Sudden Failure: Halogen bulbs have fragile filaments that degrade over time. A bulb can fail suddenly mid-surgery due to vibration (when moving the boom arm) or thermal shock. This forces the surgical team to rely on backup bulbs, creating a moment of visual disruption during critical maneuvers.
-
UV Radiation Leakage: Unlike LEDs, halogen bulbs emit a broad spectrum that includes harmful Ultraviolet (UV) rays. While filters are used, cracked or aged filters can expose both the patient’s internal tissues and the surgical team’s retinas to damaging radiation.
The LED Light: Cold, Consistent, and Safe

LEDs produce light through Electroluminescence, a process that generates negligible infrared heat in the light beam itself.
-
"Cold Light" Source: LEDs do not heat the patient or the surgeon. This preserves tissue hydration and keeps the surgical team comfortable and focused, even during 10-hour procedures.
-
Spectral Precision: Unlike the fixed spectrum of halogen (warm yellow), LEDs can be tuned. By mixing specific phosphor-coated chips, manufacturers can achieve high Color Rendering Indexes (CRI) without the waste heat.
-
Reliability: An LED surgical light typically consists of an array of dozens of individual chips. If one chip fails, the remaining matrix ensures the light field remains uniform, eliminating the risk of total blackout.
However, the shift to LED has introduced new challenges. Just like surgical shadowless lamps, they require a soft, shadow‑free, and widely dispersed beam—this demands careful consideration of LED light distribution during the design of shadowless luminaires: precise optical lenses are essential for accurate control and presentation of the light distribution.
2. Deconstructing the "Shadowless" Effect
The term "Shadowless Lamp" is somewhat of a misnomer. In the physical world, wherever there is an object blocking light, there must be a shadow. The engineering goal is not to eliminate shadows (which is impossible) but to dilute them until they are invisible to the human eye.
The Physics of Shadow Dilution
In a surgical setting, the surgeon's head or hands inevitably block some light. If the light source is small and singular (like a flashlight), it creates a large, dark Umbra—a dangerous blind spot.
To counter this, surgical lights use the Multi-Point Source Principle. By arranging dozens, sometimes hundreds, of LED chips in a circular matrix, light strikes the surgical field from multiple converging angles. When the surgeon's head blocks light from the left, the LEDs on the right fill in the shadow. This effectively shrinks the Umbra and expands the Penumbra, rendering the obstruction "transparent" to the eye.

The LED Challenge: "Ghosting" and The Multi-Shadow Effect
While the Multi-Point principle sounds simple, executing it with LEDs is optically difficult.
A raw LED is a directional point source. If you simply mount 100 raw LEDs on a plate and point them at a wound, you don't get a shadowless effect. Instead, you get the "Multi-Shadow" or "Ghosting" effect. You will see 100 distinct, tiny shadows offset from each other. This visual noise is distracting and causes eye strain for the surgeon who is trying to focus on fine capillaries or nerves.
This is where the Optical Lens becomes the decisive factor.
To eliminate ghosting and achieve a true shadowless beam, every single LED chip must be paired with a high-precision collimating lens.
-
Capture: The lens sits directly over the LED die, capturing virtually 100% of the emitted photons.
-
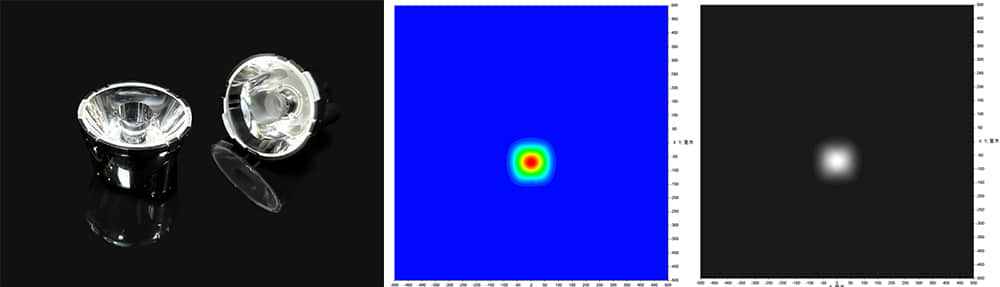
Collimation: The lens structure redirects these scattered rays into a tight, parallel beam (typically with a narrow angle like 3° or 5°).
-
Overlap (The Magic): By collimating each individual beam, the lenses allow the system engineer to mathematically calculate the focal point where all beams overlap perfectly.
When these hundreds of collimated beams converge at the surgical site (the Light Field), they mix into a single, uniform column of light. The result is a crisp, high-intensity spot with no color separation and, crucially, no distracting ghost shadows.

3. Critical Optical Metrics for Surgery: CRI, R9, and CCT
In general lighting, we measure success by "brightness" (Lux). In surgical lighting, brightness is secondary to fidelity. A surgeon must be able to instantly distinguish between a vein, an artery, and a nerve. A light that is merely "bright" but color-blind can lead to catastrophic errors in tissue diagnosis.
This is where optical metrics—specifically CRI (Ra) and R9—become non-negotiable.
The "R9" Factor: Seeing Red
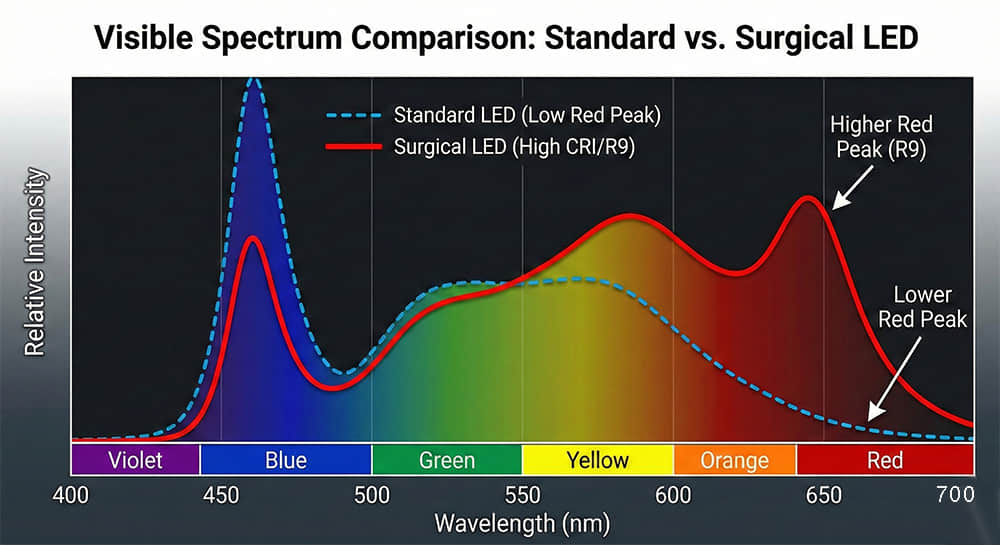
Most buyers are familiar with CRI (Color Rendering Index), or Ra, which measures how natural colors look under a light source. While a standard office light might have a CRI of 80, a surgical light requires a CRI of 95+.
However, Ra is an average of only R1 through R8—mostly pastel colors. It does not include R9, the specific metric for Saturated Red.
-
The Clinical Risk: In an operating room, "Red" is the canvas. Blood, muscles, and organs are all shades of red. If a light source has a high CRI (95) but a low R9 (e.g., <50), flesh tones will appear desaturated or greyish.
-
The Optical Requirement: To ensure accurate tissue differentiation, Asahi Optics engineers lenses that maintain high spectral transmission. We prioritize Optical Grade PMMA materials for our medical lenses because PMMA offers >93% light transmittance and does not filter out the critical red wavelengths, ensuring an R9 value of >90.
CCT: The Balance Between Focus and Fatigue
Correlated Color Temperature (CCT) is another critical tool. Modern LED surgical lights are often "Tunable," allowing surgeons to shift between:
-
Cool White (5000K+): High contrast, ideal for short, intensive tasks like orthopedic surgery.
-
Warm White (3500K-4000K): Softer on the eyes, reducing fatigue during long procedures or reducing glare on highly reflective red tissues.
The role of the lens here is Color Mixing. When a surgical lamp mixes cool and warm LED chips, the optical lens must perfectly blend these two outputs. A poor lens will result in "color separation," where the shadow has a pink or blue edge. Asahi’s micro-structured lens surfaces ensure that the mixed light is homogenous from the center of the beam to the very edge.
4. Optics Lenses Solutions for Medical Devices
At Asahi Optics, we have developed a specialized Surgical Lighting Single Lens series designed specifically for the rigorous demands of the Operating Room (OR).
The Power of Ultra-Narrow Collimation
General lenses often scatter light too wide (30° or 60°), losing intensity before reaching the bottom of the incision.
I recommend the "37.8mm 5-degree surgical light lens". By compressing light into an extremely narrow 5° beam, we maximize the Center Beam Candlepower (CBCP). This enables the surgical light to project high-intensity illumination (up to 160,000 lux) deep into the patient's body cavity without requiring the surgeon to manually lower the light head.
Matrix Design & "Shadowless" Integration
To achieve a multi-source "shadow reduction" effect, manufacturers need to integrate dozens of LEDs into a single light head. This demands the use of compact optical components without compromising performance. such as the 32 mm 5-degree (ASH31D19H5G) and the 37 mm 3-degree (ASH37D22H3G). These small-diameter lenses allow engineers to design high-density LED arrays (matrices), increasing the number of light sources overlapping at the wound site. This, in turn, mathematically reduces shadow contrast.
-
Universal Compatibility: These lenses are optimized for the industry-standard medical LEDs, including Cree XPE/XPG/XML and Nichia series, ensuring seamless integration into your existing PCB designs.
Material Purity for R9 Retention
In medical optics, the material is as important as the shape. We utilize Optical Grade PMMA for our surgical series. Unlike standard PC which can absorb trace amounts of spectral wavelengths, our PMMA maintains a transmittance rate of >93%. Crucially, it ensures Zero Color Shift. When you select a high-CRI LED chip to get that vital R9 (Deep Red) value, our lens delivers it 100% to the tissue, ensuring doctors see the true color of the pathology.
Custom Optical Design
Every surgical lamp is unique. If our standard 1.9° or 5° lenses do not match your specific focal distance requirements, Asahi Optics offers full Custom Design Services. From initial ray-tracing simulation to mold production, we can engineer a lens that perfectly matches your fixture's geometry.
5. Conclusion: Optics as a Medical Instrument
In the operating theater, there is no margin for error. As medical technology advances from the "thermal era" of halogen to the "digital era" of LED, the criteria for lighting have shifted from simple brightness to absolute optical precision.
We have learned that a high-performance surgical light is a system, not just a bulb. While the LED chip provides the efficiency and cool operation, it is the Optical Lens that delivers the Shadowless Effect, ensures Deep Cavity Illumination, and preserves the critical R9 Red rendering needed for accurate diagnosis. Without a precision lens, even the most advanced LED is merely a blinding spotlight.
Don't compromise on visibility. Equip your medical devices with optics that match the skill of the surgeons using them. Contact Asahi Optics today to discuss your surgical lighting